
Care Plan Team

You followed the list.
You avoided coffee. Spicy food. Dairy. Gluten. Tomato. Citrus. Fried foods. Maybe even some of the meals you actually love.
And somehow, your symptoms still feel confusing.
One day, a meal feels fine. Another day, something similar leaves you bloated, uncomfortable, or dealing with reflux symptoms. So you go back to the list. You cut out another food. Then another.
But the list still does not feel like your body.
That is the problem with generic trigger lists. They can be useful starting points, but they are not personal maps.
Generic trigger lists can help, but they cannot explain everything
Most trigger lists are built around foods that commonly bother some people. That can be helpful. If you are dealing with reflux, IBS, bloating, or IBD-related food confusion, it makes sense to know which foods may be worth paying attention to.
But digestive symptoms are not always explained by one food.
The fuller picture may include the amount you ate, when you ate, what else was in the meal, how symptoms showed up, and whether the same pattern has happened more than once.
A food can be common on a trigger list and still not be your trigger.
A food can also bother you once and not bother you every time.
That does not mean the list is useless. It means the list is incomplete.
Reflux shows why timing and context matter
Reflux is the familiar example.
Many reflux trigger lists mention foods and drinks like citrus, tomatoes, alcohol, chocolate, coffee or caffeine, high-fat foods, mint, and spicy foods. The National Institute of Diabetes and Digestive and Kidney Diseases notes that some people with GERD find that certain foods or drinks trigger symptoms or make symptoms worse. NIDDK also notes that eating at least 3 hours before lying down or going to bed may improve symptoms for some people who have GERD symptoms at night or when lying down.
That matters because a reflux episode may not be explained by the food alone.
Maybe the tomato sauce was worth noticing. Maybe the portion was larger than usual. Maybe the meal was higher in fat. Maybe you ate late and lay down soon after.
The better question is not only, “Was this food on a reflux trigger list?”
It is also, “What else was happening around this meal?”
IBS shows why personalization matters
IBS is one of the clearest examples of why generic lists can break down.
The National Institute of Diabetes and Digestive and Kidney Diseases notes that different diet changes may help different people with IBS. A clinician may suggest changes like adjusting fiber, avoiding gluten, or trying a low-FODMAP diet, depending on the person. NIDDK also notes that if symptoms improve with a low-FODMAP approach, a doctor may recommend slowly adding foods with FODMAPs back into the diet, and some people may be able to eat some FODMAP-containing foods without IBS symptoms.
That is an important point.
Even one of the most structured digestive-health food approaches is not meant to be a permanent list of foods to fear. The American College of Gastroenterology describes the low-FODMAP diet in three phases: elimination, reintroduction, and personalization. In the personalization phase, the goal is to avoid only the foods that bother you, which can help keep the diet balanced. ACG also notes that portion size matters, that low-FODMAP does not cure IBS, and that a trained dietitian can help guide the process.
So for IBS, the question is often not, “Is this food allowed or forbidden?”
It may be:
What portion seems better tolerated?
Does this happen every time?
Does it happen only when I am already symptomatic?
Is this a repeated pattern or a one-off reaction?
That is very different from simply living by a list.
IBD needs a careful distinction between symptoms and harm
IBD, including Crohn’s disease and ulcerative colitis, needs more caution than general digestive discomfort.
Food experiences can vary from person to person, and food choices may depend on whether someone is in a flare or remission. The Crohn’s & Colitis Foundation explains that trigger foods can cause unpleasant symptoms, but that they do not necessarily cause harm or inflammation. It also notes that everyone may have different trigger foods.
This distinction matters.
If a food seems to worsen symptoms, that is worth noticing. But it does not automatically mean the food is medically harmful, causing inflammation, or causing disease activity.
For IBD, food and symptom tracking may help someone prepare better notes for a clinician or dietitian. It should not replace medical care, especially during flares or when symptoms are severe, persistent, worsening, changing, or unusual.
What generic trigger lists often miss

A trigger list usually names possible foods.
Your actual pattern includes the context around the food.
Before you assume a food is the problem, it may be worth tracking:
What you ate
How much you ate
When symptoms started
How intense the symptoms were
Whether you ate close to bedtime
Whether the meal was higher in fat, fiber, spice, or volume than usual
Whether you were stressed, tired, dehydrated, or rushed
Whether you were already in a flare or sensitive period
Whether the same food felt different another day
Whether this happened once or repeatedly
One reaction does not prove a trigger.
Repeated patterns are more useful than one bad day.
Before you cut out another food, look for the pattern
When symptoms feel random, it is tempting to make the list longer.
Cut dairy. Cut gluten. Cut spice. Cut beans. Cut tomato. Cut coffee. Cut every food that has ever appeared in a trigger article.
But more restriction is not always the same as more clarity.
Sometimes the better first step is to ask better questions.
Did this happen more than once?
Was the portion different?
Was the timing different?
Was the meal part of a stressful day?
Did you sleep poorly?
Were you already feeling off before you ate?
The goal is not to blame every symptom on one food. The goal is to notice what keeps showing up.
That kind of pattern can be useful. Not as a diagnosis. Not as proof. But as a clearer signal that something may be worth adjusting, watching, or discussing with a qualified clinician or registered dietitian.
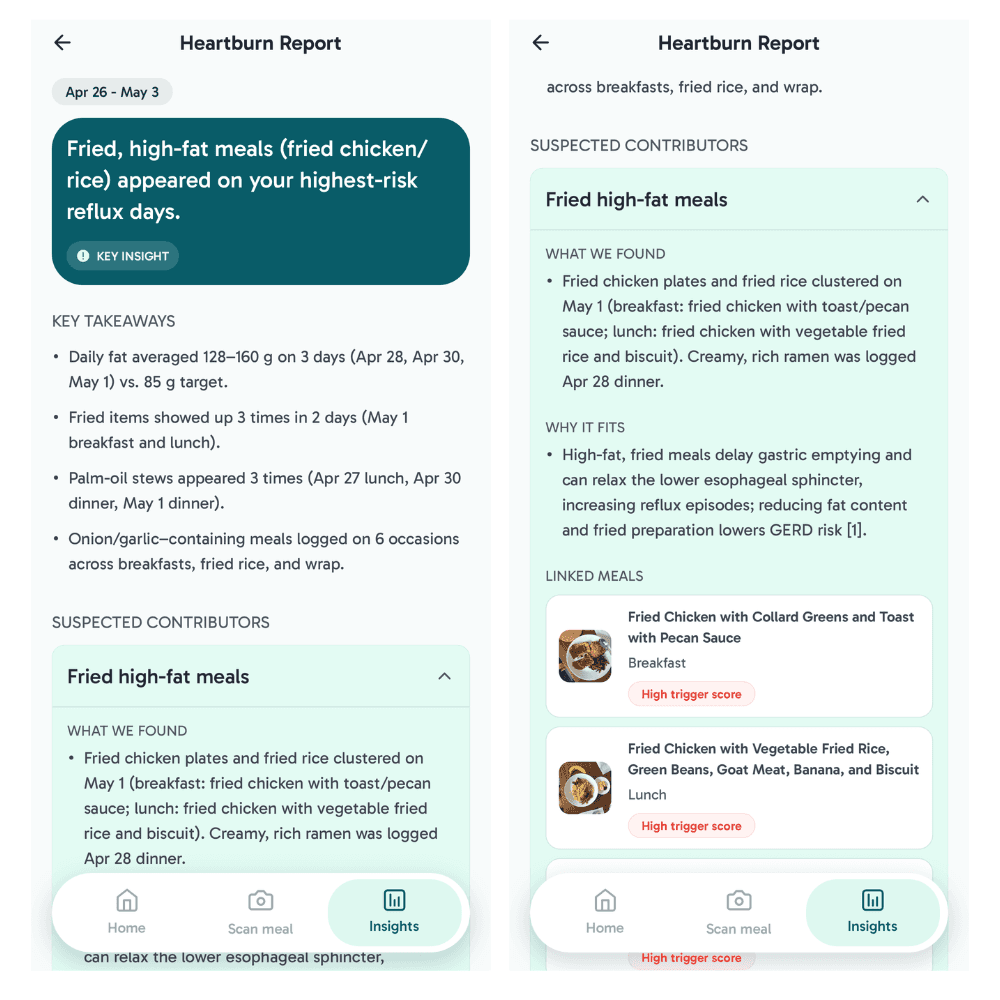
How Flourish can help you stop guessing
Food and symptom patterns can be hard to understand when you are relying on memory alone.
Flourish helps you log meals, symptoms, and health context in one place so you can start noticing possible patterns over time. It is not a diagnosis tool, and it does not prove what caused a symptom. But it can help you connect what you ate, how you felt, and what else was going on, so you are not relying on generic lists alone.
If generic trigger lists are not enough, Flourish can help you start learning from your own meals, symptoms, and daily context.
Because the goal is not another rulebook.
The goal is less guessing, more clarity.
When to talk to a clinician
Tracking can be helpful, but some symptoms should not be handled as simple food detective work.
Consider talking with a qualified clinician if your symptoms are severe, persistent, worsening, unusual, or concerning. For IBD especially, seek medical guidance for flares, blood in stool, unexplained weight loss, fever, severe pain, or worsening symptoms.
Educational note: This article is for educational purposes only and is not medical advice. Flourish is not a diagnosis or treatment tool. If your symptoms are severe, persistent, worsening, unusual, or concerning, consider talking with a qualified clinician.
Smart Eating, Better Living
© 2025 Flourish AI. All rights reserved.
Terms
Privacy
Cookies